
June 7, 2010 in INFORMS News
Advancing health care on multiple fronts
Georgia Tech’s Center for Operations Research in Medicine and Healthcare partners with other organizations on a wide range of projects aimed at improving U.S. health care system.
SHARE: PRINT ARTICLE: https://doi.org/10.1287/orms.2010.03.11
https://doi.org/10.1287/orms.2010.03.11

U.S. HEALTHCARE EXPENDITURES, at $2 trillion in 2005 and 16.2 percent of the U.S. gross domestic product, are projected to reach $4 trillion in 2015 and 20 percent of GDP. Approximately 31 percent of health care costs are administrative, 35 percent are elderly consumed, 75 percent relate to chronic disease management and 25 percent relate to spending linked to risky behaviors. These expenditures are expected to continue to be nearly evenly split between public funding and private funding. Thus, health care’s impact on the economy is substantial in relation to public spending, private funding and U.S. competitiveness in the international economy.
The medical and health care industries are fragmented and complex, have multiple stakeholders and must accommodate dynamic, rapidly changing processes.Compared to other industries, improving health care presents unique challenges. Consider, for instance, that couriers misplace one out of 100,000 parcels, but 5 percent to 10 percent of medical records are reportedly misplaced. Whereas the banking industry has a transaction error rate of one in 10 million, the error rate in hospital transactions is more than two in 100 (2 percent). The accident rate for airplane landings and takeoffs is on the order of one in one million, whereas about seven in 100 (7 percent) adverse medical events are related to the administration of medication.
Although criticism of the lack of timely research on adoption and effectiveness of innovations in health organizations dates back well over a decade, evidence of the failure to deliver has been noted more recently as well. In particular, within the Institute of Medicine, five reports have been published highlighting some of the persistent challenges. The 1999 IOM report “To Err is Human” reported that 44,000 to 98,000 Americans die each year as a result of medical errors. In fact,medical error is the seventh leading cause of death in the United States, and the costs associated with preventable adverse events range from $17 to $29 billion. The 2001 IOM report “Crossing the Quality Chasm: A New Health System for the 21st Century” highlighted that the health care system is “plagued by a serious quality gap” and called for eliminating handwritten clinical information by 2010 and refocusing the health care system on treating chronic illnesses. This led to drastic changes and active engagement of the medical community, and the development and adoption of electronic medical records for clinical operations on multiple fronts.
The 2002 report on “Leadership by Example: Coordinating Government Roles in Improving Health Care,” argued that the federal government should lead the development of clinical standards for measuring care and proposed financial incentives for organizations that improve quality. In the 2003 report on “Keeping Patients Safe: Transforming the Work Environment of Nurses,” problems in hospital, nursing home and other health care organization work environments that threaten patient safety through their effect on nursing care were identified and improvements were recommended.
The 2005 report by the IOM and the National Academy of Engineering “Building a Better Delivery System: A New Engineering/Health Care Partnership”included findings and recommendations for building a strong partnership between engineers and health care professionals to address the crises facing health care delivery in the United States. Further, it reported that the health care industry has devoted relatively little technical talent and intellectual effort to optimizing its operations (particularly at higher levels of systems – hospitals, regional networks, etc.) or to measuring its performance in terms of quality and productivity. This neglect has contributed to the development of a high-cost delivery system with poor operational processes and performance measures that provides highly uneven quality of care and limited coverage/reach of quality care.
Some of the main health care issues in the United States include gaps in access to services, patient safety and medical errors, varying levels of quality, unacceptable rates of growth in health care costs, the intrinsic Social Security and Medicare financial crises, and inefficient delivery systems that lead to poor performance and productivity. These challenges are amplified by the changing medical and health landscape: the growing cost pressures, the aging population, the growing complexity of science and technology, and the urgent need to integrate biological and computing revolutions within diagnosis and treatment to improve the clinical outcome.

conducts an experiment inside a biological safety cabinet within the Biosafety Level 3-enhanced laboratory.
Health Information Technology
The need for Health Information Technology seems to be one of the few topics upon which Democrats and Republicans agree.
IN A JAN. 8, 2009 SPEECH on the economy delivered at George Mason University, then President-Elect Barack Obama said,“To improve the quality of our health care while lowering its cost, we will make the immediate investments necessary to ensure that within five years all of America’s medical records are computerized. This will cut waste, eliminate red tape and reduce the need to repeat expensive medical tests. … it will save lives by reducing the deadly but preventable medical errors that pervade our health care system.”
The need for Health Information Technology (HIT) seems to be one of the few topics upon which Democrats and Republicans agree. Both former President Bush and President Obama set 2014 as the target date for computerizing medical records.However, a recent National Research Council report cautioned that “current efforts aimed at the nationwide deployment of health care IT will not be sufficient to achieve the vision of 21st century health care, and may even set back the cause if these efforts continue wholly without change from their present course.”
Since the 1960s, operations research has had a long and continued presence in the health care arena, especially in areas related to health policy, efficiency improvement and operations logistics. Significantly, prominent members of the O.R. community such as Bill Pierskella, Seth Bonder and others have made a lasting impact to health delivery and management, while Margaret Brandeau, Ed Kaplan and Larry Wein injected O.R. models into the public health policy arena. Today, many IE/OR departments in major universities have focused programs on health care logistics and various health-related research topics.
Despite the proliferation of papers in the academic literature and individual anecdotal success stories, major reports still highlight the barriers regarding getting O.R. techniques widely accepted and used as part of mainstream decision-making by clinicians, health managers and policy-makers. Further, because of the nascent use of standards for data interchange; privacy and security concerns; and the special interests of insurance, medical and consumer advocacy groups, a multitude of challenges must be overcome before O.R. tools can be used to their best effect. Compounding that problem, new medical and biological advances continue to demand technological advances to solve the complex large-scale problems arising in diagnosis and treatment.
This article discusses medical and health care research problems that my colleagues and I are investigating at the Center for Operations Research in Medicine and Healthcare at Georgia Tech and the Center for Health Organization Transformation, a National Science Foundation Industry/University Cooperative Research Center with which Georgia Tech is affiliated. The discussion relates to our view and experiences. We acknowledge that there are other operations researchers working on interesting medical and health care-related problems, and regretfully we are not able to acknowledge all of them here.
Health information and management of evolving clinical/biological data for advances in patient care
ONE OF THE HURDLES that must be overcome before clinical advances and process improvements involving medical information can be fully realized is the relative widespread nonuse of computerized systems for patient records.As reported in the 2001 IOM report, the lack of such systems in health care organizations contributes to medical errors that cause hundreds of deaths and tens of thousands of serious illnesses every year. Around the country, the adoption and level of use of computerized information systems for patient care within health organizations varies greatly. While some began the journey to electronic health records 20 years ago (e.g., The Veterans Administration Hospitals, New York Presbyterian Hospital), there are still many hospitals and practitioners that are just beginning the process of converting from paper records to electronic ones. If realized, the current administration’s goal of having all of America’s medical records computerized by 2014 will revolutionize the way information is stored and used.
Taking things one step further, data connectivity across distributed clinics and laboratories can help to accelerate research and translational advances for improved patient care.Within an individual health care enterprise, clinical data and electronic medical records (EMR) are often stored and managed in a centralized location through a highly secure HIPAA compliant infrastructure, whereas translational technological data related to genomics, proteomics and metabolomics are stored in distributed databases among local laboratories. These data provide different levels of detail to patient history. The combined rich collection of clinical information provides windows of opportunity to conduct largescale clinical research, data and knowledge sharing and multi-center clinical trials that can impact the practice and quality of medicine and scientific discovery.
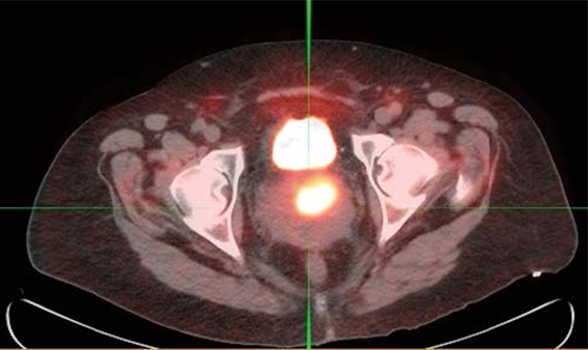
images of a cervical cancer patient. Lee and her team use such images to develop novel biological planning
and treatment strategies for improved outcome.
As part of the NCRR-funded translational and clinical research effort, and in collaboration with Emory University, Morehouse School of Medicine and Children’s Healthcare of Atlanta,we are leading the design of a software enterprise that supports and advances clinical and translational research. The software enterprise provides an inter-community-based health/clinical informatics environment that facilitates multifacility secured data access and communication, clinical trials, outpatient research, community-based research, public health research and regional clinical connectivity for optimal translational and clinical advances and training.
The connectivity software enterprise is based on a modeldriven code generation process that allows for adaptation capability to respond to required changes in evolving and expanding clinical and translational data management. Our approach builds on three basic components: storage in relational databases, application access to data through an Entity-Relational (ER) model description and a health care ontology. Given an ER model over ontology, our tools are able to generate new database schema, create the new database and generate new queries to access the new database rapidly.The adoption of a health care ontology makes the tools easily extensible as the application evolves to include more data sources and clinical areas. Experience with multiple distributed databases (involving imaging, biomarker, clinical patient record and metabolomics data) shows that the model-driven code generation is a promising approach for clinical data management systems that must evolve as the application and data sources change.
Running inside a secure HIPAA zone, the system allows clinicians access to clinical and translational data for operational usage, clinical trial patient selection, and various translational and investigative usage.Users can aggregate, analyze, mine and extract data from various databases, and test and make recommendations of health standards. For hospital administrators, such a system provides them with the means to analyze utilization, billing, planning and development. Further, for clinical investigators and researchers, the system creates data sandboxes to enable the translational research of disease modeling, algorithm development, text mining and data analytics to advance the medical decision process in disease diagnosis and prediction, optimal treatment, outcome prediction, comparison effectiveness and population health through the use of large-scale datasets.
Predicting health risk, early disease diagnosis/detection and treatment outcome prediction
ONE OF THE CHALLENGES in biomedicine involves the use of biological and clinical data to assist in health risk prediction, early disease detection and treatment outcome prediction. This has the potential benefits of increasing the odds of curing a disease (e.g., brain tumor), obtaining treatment before severe permanent damage has occurred (e.g., diabetes, inflammation, Alzheimer’s disease, macular degeneracy), improving chances of survival (cardiovascular, breast, pancreas, liver cancer) and selecting the best regime for treatment. Early detection allows for earlier intervention, thus greater chances for treatment success and recovery.
The challenges facing scientists in this pursuit is that in experimental biological and medical research, experiments are often performed under different conditions and on different molecules to reveal potential predictors for biological and medical phenomena.While there is a wealth of biological and clinical data available for researchers, there are limits on existing modeling and computational techniques to handle such heterogeneous large-scale data sets to uncover the discriminatory factors. Among O.R. researchers, O.L. Mangasarian has worked extensively on mathematical programming models for classification, especially for breast cancer diagnosis.Peter Hammer and his team have focused on Boolean and logical analysis and applied it to heart disease prediction. Multigroup classification remains {NP}-complete, and presents a technological challenge for the O.R. and computer science community. Much work has been devoted and is still needed to design effective models as well as to derive novel and efficient computational algorithms to solve these multi-group instances.
Working with clinicians and experimental biologists since 1995, we have developed a general-purpose multi-group classification modeling and software system that determines predictive rules for a wide range of biological and medical problems. These rules can assist in early disease prediction and diagnosis, identification of new target sites (genomic, cellular and molecular) for treatment and drug delivery, disease prevention and early intervention and optimal treatment design.
For one project, we have developed a classification rule to predict atherosclerosis by examining inexpensive physiological measurements, traditional risk factors and novel biomarkers. In another, we analyzed genomic data to predict abnormal methylation of certain genomic regions. (Methylation is a process that has been shown to silence genes responsible for tumor suppression.)
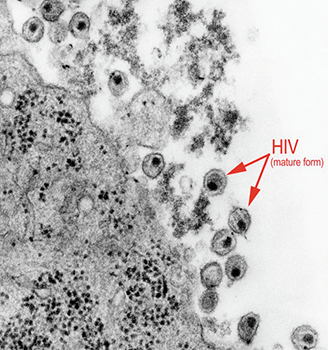
of mature forms of the human immunodeficiency virus (HIV) in a tissue sample under
investigation. AIDS is characterized by changes in the population of T-cell lymphocytes
that play a key role in the immune defense system. In the infected individual, the virus
causes a depletion of subpopulation of T-cells, called T-helper cells, which leaves these
patients susceptible to opportunistic infections, as well as certain malignancies. In
several infectious disease projects, Lee and her team of researchers study T-cell
responses to vaccine to predict effectiveness.
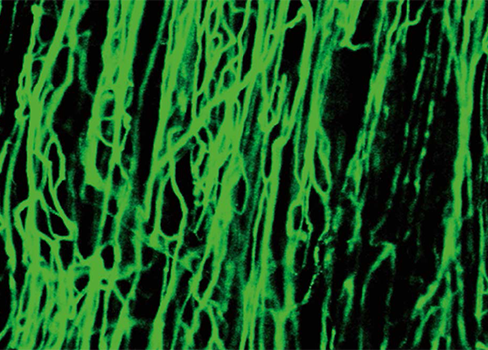
The team is also fingerprinting microvascular networks to provide early diagnosis of diabetes, aging, macular degeneration and tumor metastasis, and performing predictive analysis on cognitive behavior to detect mild impairment in order to reduce progression towards Alzheimer’s disease.
In 2009, working with researchers at the Yerkes National Primate Research Center and Emory Vaccine Center at Emory University, the teams developed a multidisciplinary approach involving immunology, genomics and bioinformatics to predict the immunity of a vaccine without exposing individuals to infection. This approach addresses a long-standing challenge in the evelopment of vaccines – that of only being able to determine immunity or effectiveness long after vaccination and, often, only after being exposed to infection.
In a wide variety of biological and medical studies, our predictive models have yielded correct classification rates ranging from 80 percent to 100 percent. The true power of these predictive rules lies in their practical usage. In all these studies, beyond reporting cross-validation results, we work with our medical collaborators and report results from blind tests (that is, predicting a new patient of unknown group identity using the developed rule). The results showed remarkable rates of correct prediction (>83 percent). This provides a strong basis for pursuing their use as medical diagnostic, monitoring and decision-making tools.
We have developed a general-purpose multi-group classification modeling and software system that determines predictive rules for a wide range of biological and medical problems.
Optimal and personalized treatment design
NEW DEVICES, imaging technologies and biological findings all pose unique challenges in their adoption within the clinical decision-making process.We use systems modeling and develop computational engines to study and investigate individualized integrative optimal treatment design. In most cases, the clinical objectives include maximizing local disease control while minimizing side effects to improve quality of life for patients. We also explore combining novel modalities and biological knowledge for cost-effective and successful outcome, recognizing that there is a need to focus on evidence-based and personalized treatment based on demographics, staging and disease types.
In one project we developed methods that account for organ motion when designing radiation treatment plans for cancer patients. Accounting for motion in image-guided treatment planning can dramatically improve under-dosing the tumor tissue and can reduce the dose to normal tissue and nearby critical healthy organs. By collecting computed tomography images over time, our team, together with clinical researchers, can track every spatial point of interest in the tumor and surrounding area during each phase of the breathing cycle. This allows us to develop treatment plans that account for breathing, motion and shape changes throughout the treatment regime in intensity modulated radiation therapy.
In lung cancer cases, this has resulted in reducing the average dose of radiation to the normal lung tissue, heart and esophagus. For liver cancer, the radiation delivered to normal liver and non-liver tissues has been reduced significantly.

In another project,we incorporated enhanced PET [positron emission tomography] signals into treatment planning for cervical cancer to boost radiation in regions of the tumor that showed dense pockets of tumor cells. Such a procedure facilitates targeted delivery of the escalated dose and the potential to improve overall clinical outcome. Expected improvements in tumor control and dose reduction to organs at risk can be significant.
Our team is studying timing and accessibility of treatment in a project involving HIV patients. Specifically,we study the tradeoffs on the timing of treatment, and its eventual societal and downstream effect and larger impact to the general population. In personalized treatment design, the objectives are complex, multiple and often competing. Very often, the biological and clinical objectives are not readily available, nor are they in explicit mathematical forms that can be easily incorporated within our modeling tools. From our experience, computational advances are ordinarily needed in order to solve the resulting treatment instances, as they are often large-scale, dense and intractable by existing commercial systems.While the work can result in significant clinical advances and societal impact to a large population,we must be patient and diligent in experimental design and clinical trials to validate our results thoroughly across different clinical sites and over a large set of patient cases.
Public health, emergency response and disaster medicine
PLANNING FOR A CATASTROPHE involving a disease outbreak or mass casualties is an ongoing challenge for first responders and emergency managers. They must make critical decisions on treatment distribution points, staffing levels, impacted populations and potential impact in a compressed window of time when seconds could mean life or death. Although extensive resources have been devoted to planning for a worse-case scenario on the local, regional and national scale, the U.S. Government Accountability Office found gaps still exist.While many states have made progress in planning for mass casualty events,many noted continued concerns related to maintaining adequate staffing levels and accessing other resources necessary to effectively respond. Our research effort began in 2003 and now includes various projects involving public health informatics and large-scale response efforts for all hazard events, including biological, chemical and radiological events, as well as infectious disease outbreaks.Much of this effort is in collaboration with the Centers for Disease Control and Prevention and hundreds of local and state public health and emergency departments. Along with CDC, we have developed a suite of computational decision support tools, RealOpt, that has been used by more than 1,800 public health and emergency response directors across the nation.
Some of our work involves:
- Strategies for designing (rapidly) effective vaccines against medical emergencies (e.g. flu vaccines, prophylactic medication for anthrax, etc.).
- Medical countermeasures dispensing: strategies for large-scale population protection. Our team has been involved in anthrax drill exercises, actual vaccination for seasonal flu vaccines, drive-through vaccination of 10,000 individuals against Hepatitis A, and H1N1 flu clinic design and mass vaccination events.
- Population monitoring and screening for radiological emergency events. Specifically our team designed community reception shelters for screening and decontamination, and studied the short-term and long-term health effect as a result of radiological events.
- Real-time decision support and strategies for effective emergency and medical response.
- Analysis of emergency communication infrastructure.
- Surge capacities (medical, public health, facility-based and community-based).
- Disease propagation analysis, mass casualty mitigation and procedural interventions.
- Clinic planning for emergency preparedness (pandemic flu clinic planning).
detection.
Modeling and optimizing public health infrastructure involve elements of resource allocation under risk, uncertainty and time pressure; large-scale supply-chain management; transportation and operational logistics; and medical treatment and population protection.The operations must be supported by an effective communication infrastructure. There is a need for vertical and horizontal integration and communication, where federal, state, local, tribal, territorial, private and business stakeholders work toward a common goal of a resilient public health system. The infrastructure must be flexible, scalable, sustainable and elastic to support an effective and timely response and to mount rapid recovery and mitigation operations.
Public health and medical preparedness continue to shower challenges on the scientific community. Some critical issues include: a) realistic systems modeling; b) intractability of largescale instances; c) inter-dependencies among multiple critical components/ agencies; and d) the importance and necessity for end-to-end systems modeling and design. Technological advances are needed to allow for complex realistic modeling while providing users with affordable computational power that result in decision systems that are practical for actual scenario-based analysis. The effective integration and alignment of care personnel, facilities, and equipment and supply for optimal outcome remains essential. Capability to solve large-scale resource allocation and location problems is a must. Tracking of disease and designing and implementing dynamic mitigation strategies will have a tremendous impact on population protection. Supply chain management needs to be dynamic, and multi-agency partnership models should be developed. Information sharing and management, and risk and communication strategies continue to evolve.Multi-modality integration of technologies and reliable platforms for communication and public dissemination are critical. Policy and coordination among different stakeholders across country borders need to be studied and potentially streamlined. While many issues relate to operational and strategic planning, many others involve policies, risk management, security, public communication, and cultural and human behavior.
Industry-University Cooperative Research Center for Health Organization Transformation
IN 2008,GEORGIA TECH and the Texas A&M Health Science Center School of Rural Public Health established the NSF I/UCRC Center for Health Organization Transformation (CHOT). Led by Larry Gamm at Texas A& M and Eva Lee at Georgia Tech, the center focuses on transformational changes in health organizations on issues related to information technology implementation, quality and safety management, chronic disease management, clinical change initiatives and other evidence-based management approaches.
There is wide-spread agreement among managers of health care organizations and policy-makers on the legitimacy of, if not strategies for attaining, all of the Institute of Medicine’s (2001) six aims for care improvement in the health systems: 1. safe, 2. effective, 3. patient-centered, 4. timely, 5. efficient, 6. equitable. The Institute for Health Improvement’s 100,000 Lives Campaign is reflective of the buy-in by hundreds of health systems in the IOM’s safety objective. Strategies for disease management and development of personal health records have reflected increased attention to IOM’s patient-centered care. Targeted efforts for the uninsured, IOM’s “equitable” target, have been reflected in the progressive federal effort in pushing forward universal health care coverage.
Current economic conditions and quality shortcomings leave little doubt that health care service organizations require transformational changes. Numerous scholars have attached varying definitions to phrases like “organizational transformation,”“ transformational changes” and “transformation.” These definitions include: “a planned change designed to significantly improve overall organizational performance by changing the behavior of a majority of people in the organization” and “to radically change traditional practices and ways of doing business.” “Profound,” “fundamental” and “modification of patterned behavior” are other words used to describe transformation. These definitions all identify a transformation as a phenomenon beyond simple innovation adoption; rather they point to efforts that change the entire operation and culture of an organization. Transformation fundamentally alters practices and culture and leads to improved health care.
The vision of CHOT is a transformed American health care system that, following the Institute of Medicine model, is safe, effective, efficient, timely, equitable and patient-centered. The mission is to advance, with its industry partners, transformation in health systems – especially in hospitals, clinics and physician groups – through cooperative applied research. CHOT’s overarching goal is to conduct cooperative research, by teaming university faculty and students with health organization management and clinical professionals, who together seek to advance knowledge and practice of transformational strategies that combine evidence-based management, clinical innovations and ongoing organizational learning.
The ability to directly inject innovative concepts into health systems and to validate and refine them for actual usage is not only exciting work, it is also of paramount importance to the health transformation process. The chain of events in patient care, from diagnosis to treatment to delivery, as well as the entire finance and organizational infrastructure, offer much room for systems advances and innovation.
CHOT consists of academic leaders, industrial leaders (health transformation leaders), program directors of the National Science Foundation and external evaluators.Research and practical transformation projects in the center cover a very broad spectrum, including: 1) organization transformation (optimizing EMR adoption, transformation sequencing, diversity management and cultural change and staff satisfaction); 2) process and delivery transformation of novel operations modeling and decision making (hospitals call centers, emergency room flow, disease management, hospital capacity and efficiency, and medical error mitigation); and 3) community and clinical care transformation (personalized and minimal invasive diagnosis and treatment, remote patient monitoring, reduction in the need and use of hospitalization, and linking long term care and acute care). The following list briefly highlights a few projects that are led by the Georgia Tech team:
- Optimal Care Delivery Model (optimizing capability and efficiency). Individual health systems provide various services and allocate different resources for patient care. In this study, we investigate optimal care delivery models for health systems through standardizing, consolidating tertiary services within the organization, and optimizing resources and demand-supply alignment for overall patient care so as to increase quality and timeliness of care, maximize financial performance, decrease practice variability
across the organization, optimize clinical workflow, and improve accessibility and dissemination venues for high-quality treatment care across a broad spectrum of the population. - Reducing Medication Errors and Cultural Transformation. This project involves a partnership between health systems leaders and Georgia Tech to design and implement a novel workflow and optimization system for medication processes. The implementation focuses on cultural and workflow transformation that aims to improve overall medication safety. The analysis aids in understanding the types, causes and impact of medication errors occurring at different stages of medication workflow. Process intervention and optimization and cultural transformation are performed to mitigate errors and improve quality of care.
- Health Information Technology and Optimizing EMR Usage (beyond adoption). Clinical data from electronic medical records (EMRs), laboratory and imaging systems, etc., provide a wealth of information for advancing diagnoses, optimizing health care delivery operations and improving patient care. Fundamental difficulties with efficient usage of clinical informatics systems include continual evolution and the inability to easily analyze large-scale distributed datasets to uncover important information for medical decisions. This project deals with health information technology to advance patient care. Our team develops medical decision-making tools through systematic modeling and analysis of clinical and health data that are generated from EMR, laboratory and imaging systems. Technologies in managing electronic alerts with human cognitive decision and preferences are designed and tested in clinical settings for routine operational usage.
- Chronic Disease Management. As both the health care costs and the number of U.S. citizens who are diagnosed with one or more chronic conditions continue to rise, unique ways of reducing costs to the public must be explored. As noted at the beginning of this article, chronic illness health care costs account for 75 percent of the $2 trillion health care budget. Reducing the occurrence of these conditions and finding ways to help patients reduce unnecessary health care provider visits can help alleviate the costs. One approach for non-delay consultation that reduces costs while providing patients with more accessible care is to create remote patient monitoring systems that can be used from the home to connect with the doctor. Our team has designed such a prototypical system that would: a) allow patients to receive more frequent interaction with health care providers; b) expand the reach and influence of health care providers to those who have difficulty visiting the doctor; c) provide a tailored approach to individualized treatment; d) promote active participation of patients in the management of their health care; e) encourage and influence healthy lifestyles; and f) and provide more accurate patient health tracking and medication compliance.
Eva K. Lee is a professor in the H. Milton Stewart School of Industrial and Systems Engineering at Georgia Institute of Technology, director of the Center for Operations Research in Medicine and HealthCare, and a codirector of the Center for Health Organization Transformation, a National Science Foundation Industry/University Cooperative Research Center. She is also a senior health systems professor at the Department of Veterans Affairs.
([email protected])