
April 3, 2020 in Healthcare Facility Activation
Advancing Mayo Clinic’s Global Strategy
Leveraging management science and engineering, famed healthcare organization facilitates successful activation of a major healthcare facility in Abu Dhabi.
SHARE: PRINT ARTICLE: https://doi.org/10.1287/orms.2020.02.15
https://doi.org/10.1287/orms.2020.02.15

Last year, in alignment with its global strategy to partner with other renowned institutions for delivering world-class patient care, Mayo Clinic was engaged to provide consulting services for a medical facility in Abu Dhabi, United Arab Emirates (UAE). The goal was to develop a successful and agile activation plan and assist in the seamless transition of patients, staff and services from the existing Mafraq facility to the new destination medical center, Sheikh Shakhbout Medical City (SSMC). The transition had to ensure high quality, patient-centered, safe and integrated care. This article chronicles the lessons learned from this unique engagement, as well as the challenges of safely and successfully activating a large, complex healthcare facility across the world and cultures in less than seven months.
Planning for SSMC began over a decade ago with a vision to be the “Hospital of the Future” and the flagship hospital of Abu Dhabi Health Services Company (SEHA), a government-run health system with 14 hospitals. With expectations high, the successful activation of SSMC was important to multiple stakeholders, including staff, patients, the Emirate of Abu Dhabi and the region. SSMC is one of the largest hospitals in the UAE with 741 beds. The goal was to replace the existing Mafraq facility (outpatient clinic and 341-bed hospital) and move clinical practices and patients into SSMC. In May 2019, Mayo Clinic signed a development agreement with SEHA to provide management and consulting services for the planning and activation of SSMC.
Strategy and Planning
The SSMC Activation Vision and Guiding Principles were co-developed by a joint Mayo and Mafraq team to ensure decision-making was driven by common goals and shared values. The joint vision aspired to successfully activate SSMC with a focus on delivering the best patient care. The following examples of guiding principles reflects the alignment of the Mayo-Mafraq team:
- The needs of the patient come first, recognizing local customs and expectations
- The activation should be designed with patient and staff safety as a top priority
- Demonstrate mutual respect and reciprocity
- Hold ourselves accountable to the highest level of professionalism and integrity
- Transparent communication among project leadership and stakeholders
- Recognize that perfection is the enemy of good
The successful execution of such a complex plan with an aggressive schedule necessitated the involvement of strong frontline staff and leadership talent. To that end, Mayo built a multidisciplinary leadership team to quickly execute decisions by drawing on the wisdom of past experience, accommodating various stakeholder needs and providing clear and frequent communications from concept to plan to execution. Staff selection criteria considered past experience and expertise, performing with cultural sensitivity, especially under pressure, and dealing with ambiguity.
Mayo Clinic’s Department of Management Engineering and Consulting (ME&C) was engaged to design and execute an activation plan for the new facility. ME&C health system engineers and a project manager participated in the multidisciplinary team with representatives from both organizations. ME&C played a key role in quickly understanding the current and desired future state, conducting a gap analysis, leveraging best practices identified through benchmarking, literature review and experience from previous engagements, and then applying engineering expertise including analytics, forecasting and modeling. This comprehensive analysis resulted in the creation of a robust activation plan for SSMC (see Figure 1).
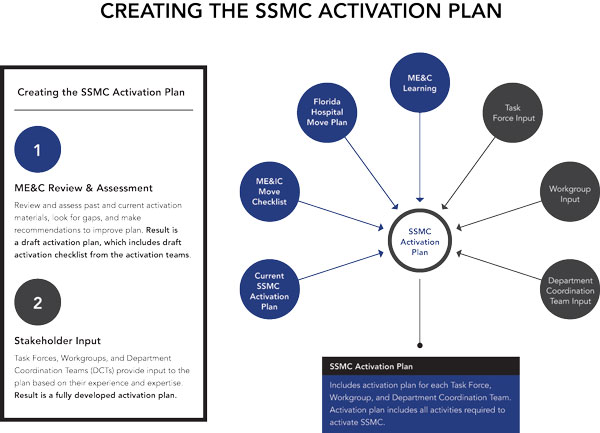
The gap analysis identified the need for clear, shared activation goals, an integrated, comprehensive activation approach, dedicated project management and systems engineering resources, and a robust change management and communications strategy. ME&C, in partnership with Mayo and SSMC team members, created a strategy and framework to facilitate a patient-centered, safe and efficient activation. The collaborative efforts of various teams produced a fully integrated and contextually aligned SSMC Activation Plan.
Crucial to success was a well-defined leadership and governance structure that provided the project with key leaders, functional committees and oversight teams representing Mayo, SEHA and Mafraq. Empowerment guidelines were created to include criteria and thresholds for decision-making at the team, department, committee and executive level. A path to escalate decisions through the governing committees and executive leadership was also defined.
Activation Structure
An activation structure (Figure 2) was designed to ensure the integration and coordination of activities across all groups. The structure leveraged best practices from previous Mayo facility activations. Physician, nursing and administrative leaders were identified from each organization to partner in leading these groups.
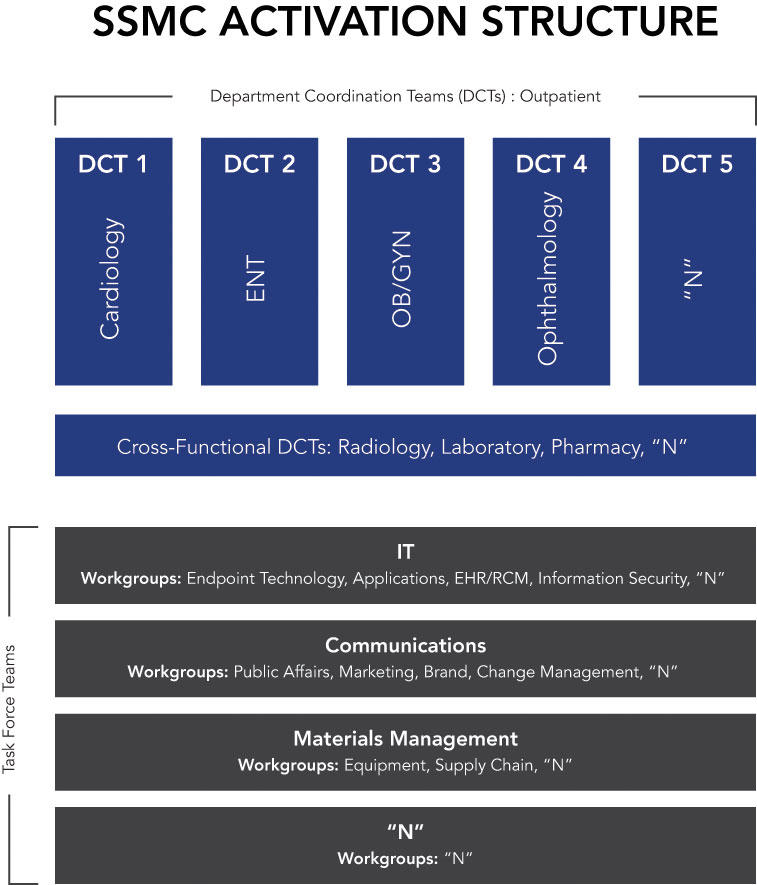
Clinical department coordination teams (DCTs), cross-functional department coordination teams (XDCTs) and task force teams (TFs) were responsible for ensuring timely completion of activation checklists, planning and executing integrated and team-specific dry runs, demonstrating progress, escalating issues and coordinating integrated workflows.
Determining the order of activation for more than 40 clinical practices was required early in the project. Attributes such as patient volumes, acuity and complexity, and practice leadership readiness were evaluated to prioritize and sequence activations. Risk analysis led to the recommendation of a staged approach with six individual activations rather than a single activation for all practices and services. The staged approach allowed practices with a high level of readiness, smaller volumes and lower acuity patients to transition first. This reduced the risk of adverse events and tested systems, processes and procedures prior to activation of more complex clinical services. However, the drawback of a staged approach involved maintaining ancillary services in two locations. These services had to modify their activation checklists to ensure high-quality and timely service at two sites. They also had to identify the ideal time to complete their transition.
Activation Preparation
The Mayo activation checklist, which had been used to successfully manage other facility transitions and activations, was leveraged to create a baseline SSMC activation checklist. The Mafraq teams enhanced the content with local knowledge and expertise. The resulting checklist was used to monitor task completion, identify and mitigate barriers and ensure that key dependencies among the DCTs, XDCTs and TFs were recognized.
Communication across various organizations was complex with diverse stakeholders. Mayo Clinic and SEHA leaders joined public affairs experts to oversee and coordinate communications leveraging content provided from multiple sources. Timely, bilingual communication regarding decisions and recommendations to work groups and staff was required to facilitate the successful completion of activation activities. Culturally sensitive communication to patients and the public was also crucial, using multiple locally relevant delivery mechanisms.
Time spent in meetings was balanced with project work, clinical patient care and administrative duties. A meaningful meeting cadence supported the activation schedule and addressed dependencies on other teams while recognizing the 9- to 10-hour time zone differential. Five meeting types addressed team dynamics and various stakeholder communications:
- Working group meetings focused on questions, issues, data analysis and solutions.
- Leadership meetings were used to evaluate options and render decisions to resolve issues.
- Project status meetings focused on critical issues, key accomplishments and important findings.
- Staff town hall meetings allowed executive leaders to communicate progress, timelines, key messages and answer questions.
- Go-live readiness meetings were held four and two weeks prior to activation to assess key tasks, critical issues, high-impact risks, interteam dependencies and interventions.
Formal logs documented, tracked and managed issues and risks. It was important to build trust and create a safe environment to encourage accurate, timely and transparent reporting. Issues and risks critical to activation were prioritized and received immediate attention and resources. Teams were encouraged to quickly report issues with long lead times (e.g., facility, equipment and short supply resources) so that aggressive mitigation plans could be created, monitored and executed.
Change management was tailored to facilitate staff engagement and build excitement. Objective measurement of staff readiness to move was assessed through baseline surveys administered prior to each activation. Questions probed for communication needs, availability of equipment, tools and technology and adequacy of training. Survey results were used by individual units to target final communications and preparations. A post-activation assessment was conducted to gather information regarding readiness and additional needs. These insights helped to inform subsequent activations.
A command center structure was created by local leadership to leverage their experience and align with the needs of the environment. The command center provided direction and oversight of activation activities, coordinated efforts to minimize risk, ensured patient, visitors and staff safety, and facilitated effective communication across all internal and external entities. Patient census was carefully managed to reduce risk and ensure safe, timely patient transfers. A Command Center Playbook guided outpatient and inpatient transitions and included the structure, roles and responsibilities, operational processes and communication strategy. The playbook provided education and training to staff involved in the transition. During each activation, ME&C supported teams by observing patient and staff flow, reporting challenges to the command center and recommending solutions for high-priority challenges.
Robust dry runs were designed to assess operational readiness and validate redesigned workflows. Integrated dry run scenarios developed collaboratively with Mayo, Mafraq and SSMC subject matter experts simulated end-to-end patient journeys and involved multiple teams. These modeled and live simulations assessed staff workflow and patient flow from the point of patient arrival to the facility and their departure. Simulations were also run for high-risk situations including emergency codes, emergent transfer of outpatients between facilities, transfer of inpatients using five distinct ambulance routes, and systems outages. Information technology created test patients to match the personas identified for the simulation.
Team-specific scenarios validated focused practice processes and ancillary functions. ME&C conducted a series of workshops to introduce the dry run methodology, its critical components and guiding principles. Scenario templates were drafted and enabled the script development process. Process owners were required to document desired outcomes and the setup, equipment, technology and education necessary to achieve the outcome for each scenario. Scenario script development was complex and contextual, and depended on the contributions of Mafraq DCT, XDCT and TF leads and subject matter experts.
Executing dry runs involved local outpatient and inpatient physician, scheduling and debrief leads. Additional representatives included multidisciplinary staff relevant to each clinical practice. Immediate debriefs were held following each scenario, and comprehensive debriefs were held after completing a group of scenarios. Dry run findings were compiled, prioritized, assigned owners and given target completion dates. Local coordination teams instituted daily huddles to track and assure resolution of findings.
Collectively, 82 integrated scenarios and more than 100 team-specific scenarios were conducted, and 320 findings were identified and prioritized (see Figure 3).
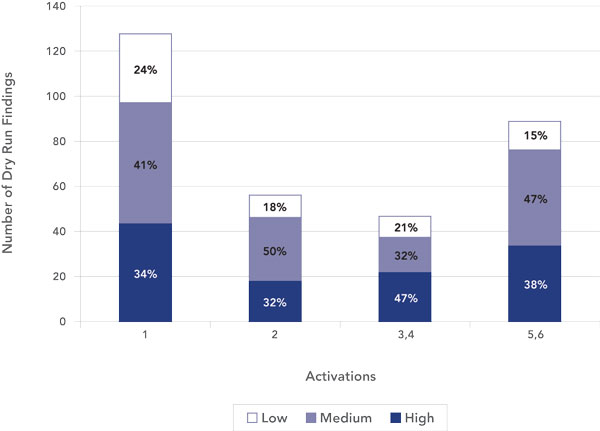
Two weeks following dry runs, 71% of the findings were resolved, 12% were no longer applicable, 7% were in progress, and 10% were prioritized as post-activation projects.
In planning for the activations, it was important to forecast the number of outpatient appointment slots that would be feasible to accommodate with staff working in a new facility and how quickly full volumes could be resumed. Timing studies and forecasting the number of inpatients that could be accommodated were also conducted, providing data for the volume of patients, number of ambulances and time needed for transfer. Based on this analysis, a detailed census reduction strategy was developed, and routine appointments, voluntary procedures and elective surgeries were reduced to allow staff to assimilate in their new work environment while ensuring the safety of patients. Staffing plans were developed and aligned to the volume and acuity of patients.
Results
To measure the success of each activation, the command center established a set of key performance indicators (KPIs) and associated metrics. The primary metric of success was patient safety. Metrics were tracked and used to determine when the command center could hand over hospital operations. Inpatient and outpatient KPIs included:
- Significant patient safety issues
- Significant regulatory or compliance issues
- Major security events
- Patient, family and staff experience
- Adverse media coverage
 Upon completion of SSMC activation, no significant patient safety issues, regulatory findings, security events or adverse media reports were found. Outpatient satisfaction was captured in the pharmacy area (typically indicating the end of the outpatient journey). Initial data reflected more than 95% patient satisfaction with clinical care, facilities and other components of their experience.
Upon completion of SSMC activation, no significant patient safety issues, regulatory findings, security events or adverse media reports were found. Outpatient satisfaction was captured in the pharmacy area (typically indicating the end of the outpatient journey). Initial data reflected more than 95% patient satisfaction with clinical care, facilities and other components of their experience.
The early activation timeline projection was several months. To limit operating two facilities with constrained resources, project leadership reduced the activation timeline to 67 days. The project timelines were met for all activations with no delays or extensions. Additionally, the command center closed earlier than expected for all activations.
Operational Transition
Operational owners were identified and engaged early, allowing active participation the in planning and activation to ensure the smooth transition of ownership from project to operations. The operational hand-off plan involved:
- operations control transitioned from the command center to the practice areas;
- issues log moved from the command center to the project management team for progress monitoring; and
- ongoing optimization and next steps transferred to the joint venture teams.
Key Lessons Learned
The valuable learnings from this large, complex international engagement are summarized as follows:
- A multicultural environment benefits from face-to-face interactions to enhance verbal and nonverbal communication. The deliberate blending of people and cultures into a cohesive team is imperative. Leadership and team members need to recognize differences and integrate them into a common understanding with expectations of how the team will function (establishing norms), collaborate, communicate and perform to meet objectives. Multidisciplinary team members from all participating organizations must be accountable for their work and contribute to team success.
- Blending the strength of diverse cultures and talent with multicultural backgrounds contributes to successful results.
- Establishing trust enables accurate reporting, sharing concerns and creative problem-solving, which are critical to successful activation.
- An on-site presence from the engineering and consulting group is essential for timely demand forecasting, root cause analysis, rapid tests of change, process mapping, solution development and effective project management.
- Digital tools (e.g., mobile phone messaging application and a common file-sharing location) established at the onset of international projects (recognizing government guidelines and technology limitations) facilitate agility in communication and decision-making.
- The creative structure and empowerment of DCTs, XDCTs and TFs enables an agile, effective “team of teams” approach [1]. This helps to break down hierarchy and bureaucracy to enable transparent communication with decentralized decision-making authority.
- Core team daily huddles are critical for timely, in-depth understanding of business requirements and effective interventions.
- Dry runs are crucial to test activation components including core clinical and business processes, as well as patient and staff experience. Conducting simultaneous dry runs adds complexity and exposes findings that stand-alone dry runs do not.
Conclusion
It was a unique and rewarding opportunity to partner with an international healthcare organization to plan and activate a flagship facility of the future. May Clinic had experience activating large, complex facilities in the United States. The SSMC engagement across the world enabled SEHA, Mafraq and Mayo Clinic to advance their capabilities to successfully activate a patient-centered, futuristic care facility. Blending management science and engineering with business and healthcare expertise in a culturally sensitive manner enabled a seamless activation, safe patient transfer, enhanced staff engagement and a sustainable operational transition from which to pursue the long-term vision.
Acknowledgment
The authors acknowledge the significant contributions of the SSMC Activation team members, subject matter experts, leaders, dry run participants and other colleagues across Mayo, SEHA and Mafraq.
Reference
- McChrystal, S.A., Collins, T., Silverman, D., and Fussell, C., 2015, “Team of teams: new rules of engagement for a complex world,” New York: Penguin Publishing Group.
Amerett (Amy) Donahoe-Anshus, M.A., is a unit head in the Mayo Clinic Department of Management Engineering and Consulting (ME&C) and an assistant professor of Health Care System Engineering and an instructor in physical therapy in the Mayo Clinic College of Medicine and Science. Janine R. Kamath, M.A., MBA, is chair of the Mayo Clinic Department of Management Engineering and Consulting (ME&C) and an assistant professor of Health Care System Engineering in the Mayo Clinic College of Medicine and Science. Arnold Blauert Jr., PMP, is a senior project manager in the Mayo Clinic Department of Management Engineering and Consulting (ME&C). Muna Khan, M.P.H., MBA, is a senior principal health systems engineer in the Mayo Clinic Department of Management Engineering and Consulting (ME&C). David O’Brien, MBA, is a senior health systems engineer in the Mayo Clinic Department of Management Engineering and Consulting (ME&C). Devin Roloff, MBA, is a senior health systems engineer in the Mayo Clinic Department of Management Engineering and Consulting (ME&C). Nina Sargent, is a senior health systems engineer in the Mayo Clinic Department of Management Engineering and Consulting (ME&C). Hugo Pariseau, M.S., is a health systems engineer in the Mayo Clinic Department of Management Engineering and Consulting (ME&C). Chris Schieffer, M.E., is a section head in the Mayo Clinic Department of Management Engineering and Consulting (ME&C) and an assistant professor of Health Care System Engineering in the Mayo Clinic College of Medicine and Science.







