
May 1, 2017 in Healthcare Analytics
Evolution of data organizations in healthcare
SHARE: PRINT ARTICLE: https://doi.org/10.1287/LYTX.2017.03.10
https://doi.org/10.1287/LYTX.2017.03.10
The big news for the Affordable Care Act (ACA) in March was the failure of the alternative healthcare bill on the House floor. For the first time since the election campaign season began, we heard real conversations between politicians and their constituents about healthcare. The uproar about healthcare in recent times made us confront the age-old question in the United States: Is healthcare a right or an entitlement?
Despite the healthcare dialogue during and after the campaign, we’re still struggling to find an answer. The ACA didn’t address this directly, although it reduced the percentage of uninsured people nationwide. Surely it increased the cost initially for the insurers, but the overall healthcare cost showed a slower rate of increase during the last few years. The expectation was that over time, the total cost would be lowered as high-utilizers of healthcare resources would get access to their healthcare at lower-cost delivery centers such as primary care office visits rather than at higher-cost hospital emergency rooms. Many times, those higher-cost episodes were also uncompensated, causing an increase in cost for paying customers and eventually to the insurers. Insurers, in turn, increased their premiums for all customers, individual or group purchasers, to recoup their losses.
Emergence of the Chief Data Officer Role
Regardless of the policy and politics, data has become the king in all industries, including healthcare, as organizations worldwide have added the role of a chief data officer (CDO) at a rapid rate the last few years. Gartner predicts that this trend will continue. However, the definition of the role is still not well articulated in healthcare. Some organizations have a CDO and a separate chief analytics officer (CAO). Others have fused them into one. The nascent CDO position faces challenges due to role ambiguity.
To understand the landscape better I recently attended a summit for CDOs. Event organizers invited leaders in data and analytics from various industries to an informal setting to discuss their challenges and successes. Attendees from different healthcare organizations, which are at different levels of maturity in terms of using data for their business, participated in several roundtable discussions on a range of issues. In this article, I will underscore some of those core topics that participants described as critical to achieve sustained competitive advantage for their data organizations.
Where Does Data Fit in Organizational Structure?
As companies continue their pursuit of transforming themselves, boardrooms are embracing the concept of data as a strategic asset. However, most industries struggle to identify the appropriate reporting structure for a data organization. Some companies place it under Marketing, some under IT. Others choose Operations or Strategy. Even within the same industry there is no common pattern.
Typically, healthcare organizations build data and analytics departments under the supervision of Clinical or IT depending on the organization’s perception of data. If it perceives data and analytics as a primary tool for clinical quality improvement, a Clinical silo is the best fit. If it is considered as another technology, then IT is the chosen silo. None of these structures, however, does justice to the role of data and analytics.
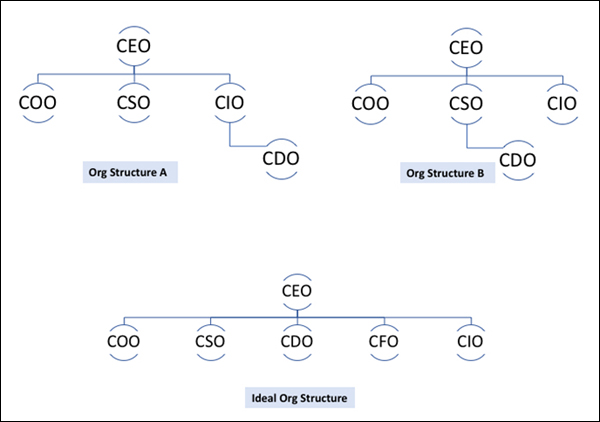
In my opinion, data organization in healthcare should directly report to the CEO. Operations, Finance, Marketing, Strategy and Clinical – all silos of a healthcare organization – benefit from using data and analytics as a transformative tool. Some organizations have started to create a new structure where the data and analytics department is part of the Office of Transformation, which reports to the CEO. That makes more sense to me. After all, organizations can transform themselves using data to become customer-driven, operationally excellent and more profitable with a sustained effort to do the right things at the right time. In many cases that also includes correctly predicting their future. This can’t be achieved without the data organization having a direct link to the CEO (Figure 1).
Centralized vs. Federated Model for Data and Analytics
Most organizations, especially large ones, operate in a hub and spoke model. Regional entities, satellite offices or sister organizations all prefer to stay independent especially when it comes to managing their own data and building analytics for their business units. This is also true in large health systems. However, having centralized governed data sources and analytics programs has its benefits.
So how do we balance the desire for a loosely coupled federated structure with the advantage of economy of scale of a centralized model? There is no easy answer to this question. Organizations have taken different approaches to resolve such conflicts. Some keep the data stewardship function decentralized, while higher-cost functions such as data science or data visualization are maintained centrally. Some organizations have adopted a hybrid approach, where most functional roles are duplicated while keeping the scope of the work of different units from overlapping. Healthcare organizations have adopted all the above.
Is Data Governance Required in the Big Data World?
Some organizations that deal with big data raise questions about the importance of the data governance functions such as data quality analysis or data stewardship. With big data, the quality of individual data elements does not matter as much it does for “small data” environments. In healthcare, most use cases are based on small data sets and, therefore, the importance of data governance and data quality management is high.
Regardless of the size of the data, some key functions of data governance such as data validation and data access policies and procedures are important for any organization, especially healthcare. This is becoming even more important as healthcare delivery organizations are becoming larger in size with ongoing merger and acquisition activities. “Region and corporate,” or the “hub-and-spoke” model, is quite common for health systems. Large organizations such as Kaiser Permanente and Sutter Health are prime examples. Leaders of both organizations consider data governance a foundational building block for their analytics programs.
ACA dodged the bullet in March, but the political firing will continue as the congressional reform effort rolls on. As a result, the healthcare industry, both payers and providers, will experience uncertainty. In the end, I am sure that all parties will accept the fact that healthcare in the United States is too complex to dramatically change. Many questions remain unanswered. Despite that, the CDO summit showed me that the enthusiasm to deal with the organizational challenges of data and analytics remains as high in healthcare as it is in other industries that are not facing such uncertainties. That is reassuring. Our data journey is very much on – rain or shine.
Rajib Ghosh is the founder and CEO of Health Roads, LLC, a consulting company for enabling digital transformation in healthcare organizations. He has 25 years of technology experience in various industry verticals where he had management roles in software engineering, data analytics, program management, product management, business operations and strategy development. Ghosh spent a decade and half in the U.S. healthcare industry as part of a global ecosystem of medical device manufacturers, medical software vendors, telemedicine and telehealth solution providers. He’s held senior positions at Hill-Rom, Solta Medical and Bosch Healthcare. His recent work includes leading data-driven digital transformation in the public health space, including county-level healthcare agencies and organizations focused on underserved populations.
([email protected])