
February 28, 2019 in Healthcare Analytics
After 10 years of innovation, what’s next?
Healthcare in the post-ACA era: What initiatives should stay, what should go in 2020 and beyond?
SHARE: PRINT ARTICLE: https://doi.org/10.1287/LYTX.2019.02.11
https://doi.org/10.1287/LYTX.2019.02.11

In a year from now, we will conclude the second decade of the new millennium. In 2010, when the Affordable Care Act (ACA) was signed into law, the U.S. Department of Health and Human Services allocated $10 billion to fund initiatives that would promote innovation in healthcare both in care delivery, as well as in payment models. Under the leadership of the Center for Medicare and Medicaid Services (CMS), the CMS Innovation Center was given 10 years and $10 billion to prove its worth.
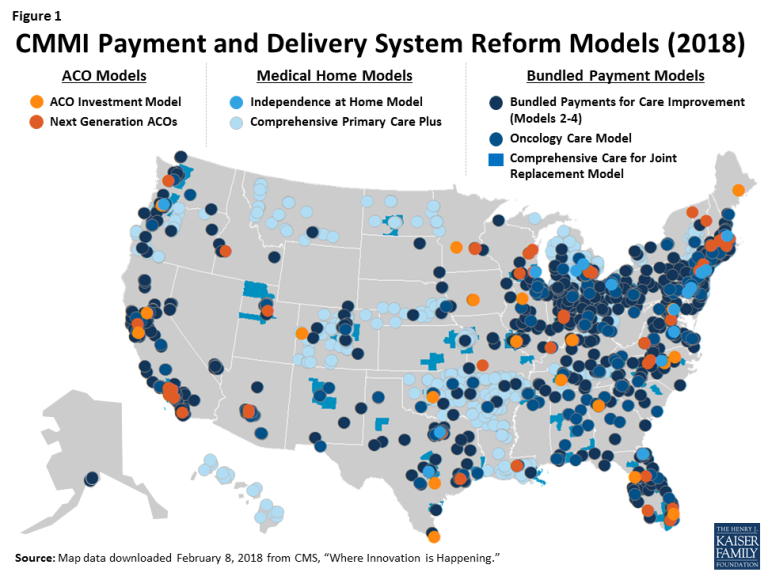
Powered by the funding, many significant transformational initiatives came out of the Innovation Center, including a new organization model for care delivery and payment called the Accountable Care Organization (ACO). In 2012, CMS launched a program called Pioneer ACOs that was comprised of 32 innovative and forward-looking healthcare organizations around the country. The result was quite impressive both in terms of cost savings as well as improvements in efficiency in care delivery. The CMS Innovation Center also started other payment model experiments called “bundled payment,” as well as primary care transformation models to test new paradigms in healthcare (see Figure 1).
On Jan. 1, 2016, CMS started the next phase of the ACO under an initiative called Next Generation ACO model with 51 ACOs. This phase tests if greater ACO accountability focusing on more financial risk bearing, consumer benefit management and consumer engagement can collectively accelerate and sustain improvement in healthcare value. The five-year testing phase will end in 2020.
All those initiatives created a huge opportunity and marketplace for healthcare analytics that never really existed before. Healthcare organizations were initially slow to react to the initiatives, but momentum picked up, which in turn propelled digitization of healthcare data in large scale. As we enter the last stage of this decade-long “innovation” period, as an active professional in this area I wonder what’s in store for the industry in the next decade. Innovation should never stop, but possibly after a decade some of the transformational innovations should either become industry mainstays or disappear altogether as unsuccessful or unsustainable. In this column, I would like to explore what I think should stay and what shouldn’t.
Electronic health records (EHR) will continue to be the main IT system for provider organizations. One of the key transformational change that ACA brought to the healthcare IT industry is the proliferation of EHR systems using “Meaningful Use” funding. This initiative incentivized physician organizations in the physical health space to adopt an EHR system and get paid for “meaningfully using” the system to electronically record patient data and sharing with each other. As a result, the number of physician practices using basic EHR for patient data recording rose from under 25 percent in 2010 to about 86 percent by 2017.
Population health management (PHM) will continue to be a key initiative. PHM will continue to drive care quality improvement initiatives. PHM is not a concept that was introduced by the ACA or CMS Innovation Center, but certainly the changes in the payment models and the introduction of the associated programs both in the Medicare and Medicaid sectors accelerated adoption of PHM as a key component of care delivery transformation. PHM goes hand in hand with strong data analytics. As a result of PHM, we have seen rapid growth of healthcare analytics from descriptive (or post-mortem of what has happened in the past) to predictive analytics. While prescriptive analytics is not yet prevalent in a meaningful way, predictive analytics is now a mainstay for many organizations.
There is no going back on this as the value of predictive analytics has been widely realized in the healthcare industry. That’s why the provider, payer and pharmaceutical sectors are all about predictive analytics like never before. As the power of analytics continue to improve and artificial intelligence technology and algorithm continue to become smarter, PHM will become better overall and drive care delivery transformation.
Multi-stakeholder care delivery with coordination will continue to proliferate. As I have written in this column before, healthcare continues to evolve from episodic care to a continuum of care. The success of ACOs has given the industry evidence that in order to keep people healthy and reduce the cost of care, it is important to consider coordination of care delivery among multiple disparate organizations. Monolithic care delivery housed in a large hospital building is not going to work for the population that the hospital serves.
A congestive heart failure (CHF) patient will likely come back to the hospital within 30 days of discharge if the post-acute care is not properly done at the skilled nursing facility, at home or at the primary care facility. If medication adherence is not properly managed post-discharge, the patient will continue to be a “frequent utilizer” of healthcare resources at high-cost facilities. This has given rise to what is now called “complex case management” where patients with high risk of readmissions are actively followed by “care coordinators” to ensure that such costly episodes of healthcare utilization are minimized with timely intervention.
Predictive models are proving to be instrumental for ACOs to proactively manage such patient cohorts by timely deploying an adequate amount of low-cost resources. This model will not only continue but proliferate in all segments of healthcare powered by healthcare analytics and care coordination software platforms.
Cost containment in healthcare can’t be sustained without a major antitrust regulation overhaul. Despite all the payment model transformation initiatives, cost containment in healthcare will not be possible if the current pace and model of industry consolidation continues. In the name of being efficient with infrastructural costs including IT costs, we have seen rapid growth in vertical and horizontal mergers and acquisitions in the hospital and physician group space. Realizing that monolithic hospital-based care delivery will be a thing of the past, hospital systems in many markets rapidly acquired physician practices, thus removing competition. Larger hospitals also acquired smaller hospitals to increase their footprints and their pricing power.
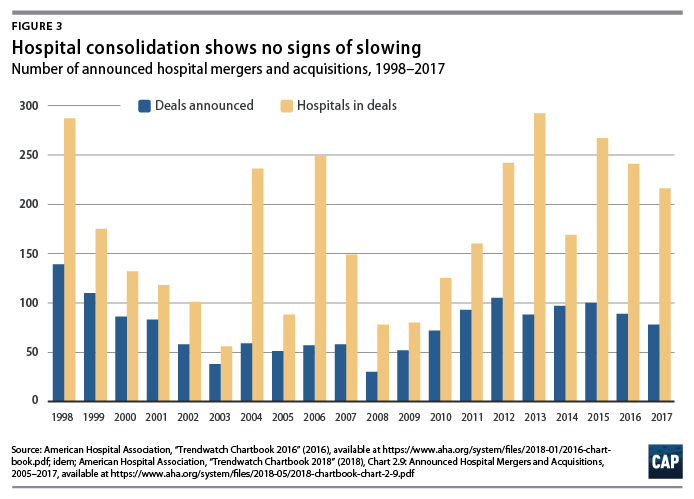
As a result, larger hospitals have been able to negotiate better payment deals with payers, while squeezing money out of those who are under- or uninsured. The federal antitrust regulations could not stop this rapid consolidation owing to many inherent issues of the regulations. For example, a group of smaller transactions such as the purchase of several small physician practices by a larger hospital system would not show up on the radar of regulators, but it could have huge consequences on the pricing of delivered services in a certain market. CMS Innovation Center’s experiments with payment models or any amount of healthcare analytics would not produce a change in the next decade unless regulators look at this issue seriously.
Physicians will not become obsolete and improved efficiency won't trump empathy. Seven years ago, Vinod Khosla, the legendary Silicon Valley investor, wrote in a TechCrunch article that 80 percent of physicians will become obsolete soon. Almost a decade later, patients are still seeing doctors. Google Health has disappeared, IBM Watson is under serious scrutiny and digital health companies are yet to produce disruption that they had promised.
The role of a physician in healthcare is often misunderstood. They play the role of a healer, which a machine cannot. Efficiency is not the word a cancer patient and his or her family members have on their minds when they see a doctor. It’s the magic words of empathy that heal the pain of impending loss. Until algorithms produce that empathic mind that heals, physicians will exist and continue to play a vital role. The next decade will surely see smarter analytics supporting physicians, but it won’t trump empathy.
Rajib Ghosh is the founder and CEO of Health Roads, LLC, a consulting company for enabling digital transformation in healthcare organizations. He has 25 years of technology experience in various industry verticals where he had management roles in software engineering, data analytics, program management, product management, business operations and strategy development. Ghosh spent a decade and half in the U.S. healthcare industry as part of a global ecosystem of medical device manufacturers, medical software vendors, telemedicine and telehealth solution providers. He’s held senior positions at Hill-Rom, Solta Medical and Bosch Healthcare. His recent work includes leading data-driven digital transformation in the public health space, including county-level healthcare agencies and organizations focused on underserved populations.
([email protected])