
June 22, 2020 in Healthcare Analytics
Pandemic exposes vulnerabilities in healthcare industry
But it will also catalyze much needed changes in public health
SHARE: PRINT ARTICLE: https://doi.org/10.1287/LYTX.2020.04.12
https://doi.org/10.1287/LYTX.2020.04.12

What a tumultuous few months we’ve been through since March! All projections that I alluded to in my last column are now obsolete. In the last two months, the United States secured the top rank in the world in terms of number of positive coronavirus cases, number of people who lost their lives to the virus, and the number of people who lost employment or income due to the pandemic. We have seen denial of the pandemic in other countries, for example, Brazil, the United Kingdom during the early days of the pandemic and Mexico, but the drama that unfolded in the United States for the last few months was unparalleled. Being a large country with a diverse population, deeply polarized political landscape and inequitable distribution of health conditions, resulted in severe loss of human lives and economic opportunities.
The responsibility to provide adequate response to the pandemic was left to the states, local authorities, businesses and even ordinary citizens with very little federal coordination. Lagging testing capabilities became a barrier to a “test, trace and isolate infected patients” strategy, causing the disease to widely spread.
The country went through shelter-in-place for weeks and even months in some places, causing small- and medium-sized businesses to furlough or lay off employees or file for bankruptcy. Congress passed an historic $2 trillion CARES Act to provide paycheck protection loans to businesses of all sizes and $1,200 one-time payment to Americans who earned less than $75,000 per year. For a family of four with two dependent children earning less than $150,000 per year, it amounted to $3,400. That provided some relief, but still the economic toll was severe. According to the updated data from the Bureau of Labor Statistics, unemployment reached about 19.7% at the end of April. In May, 2.5 million jobs were added causing the updated unemployment to come down to 16.3%, still a very sobering number that matches that of the 1930s Great Depression.
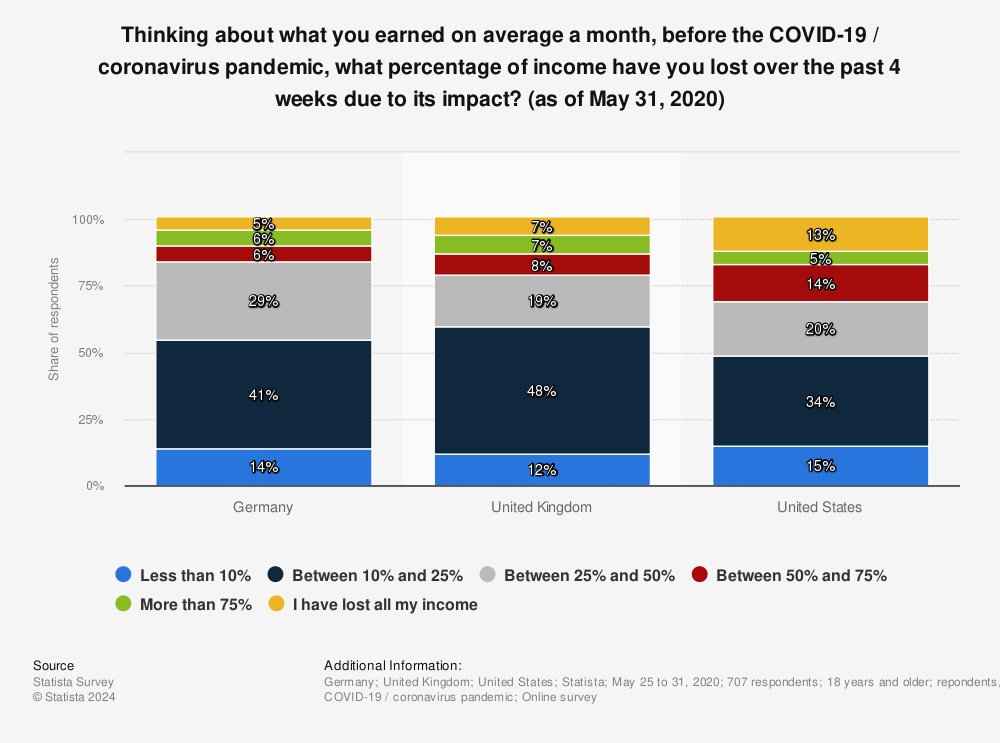
Figure 1: Income loss survey results in the United States, United Kingdom and Germany.
Based on a survey of 707 adult responders, Figure 1 suggests that compared to other large industrialized economies like Germany and the United Kingdom, the percentage of responders who lost half or more of their income due to the pandemic is higher in the United States. The wealthy 15%-20% of the population didn’t suffer much income loss other than restricted movement in all three countries. But compared to the U.K. and Germany, a large swath of the middle class and lower income population in the United States suffered major income loss. The ugly inequality of wealth distribution, and lack of enough safety net in the U.S., became evident during the pandemic. Additionally, when we analyze the death rate by race, we also see the manifestation of health inequality. In percentage terms, the African American community suffered the brunt of the virus, but in terms of absolute count, the white population suffered more deaths. But it is the percentage that matters in understanding the widespread pattern. Scarce access to quality healthcare coupled with lack of safe shelter and food insecurity among the low income and vulnerable population has been blamed for the high percentage of severe complications and deaths in the non-white communities.
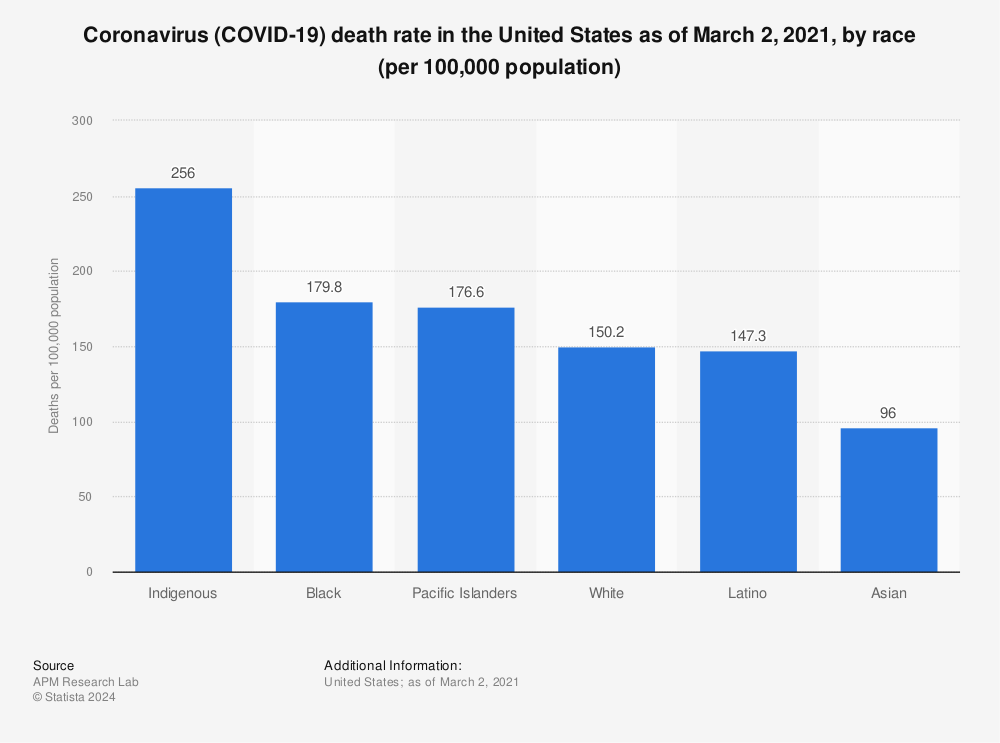
Figure 2: Death rate by race for COVID-19 in the United States as of June 9.
Reopening of the Economy: A Double-edged Sword
The rush to reopen stressed economies and bring workers and consumers back to “normal” has caused anticipated spikes in COVID-19 infection cases in several U.S. states, raising concern about an early “second wave.” The virus actually never left. The rise and ebb of virus infections were just following different curves in different places, but we are still in the first wave. What will happen if this spike increases further? In absence of a working vaccine or cure, the only intervention that has proven to have worked is social distancing of human beings and rigid adherence of the public to that protocol. We have seen massive deviations in public behavior from the recommended safety practices nationwide, reinforced by behaviors of partisan politicians.
Pausing the economic activities again might not work, but will the consumers retrench to safety if the public health crisis deepens again? After all, people value their own lives as well as that of their family members. Australian bioethics professor Peter Singer has proposed an interesting opinion in his latest writings and interviews. How many deaths can a country tolerate to keep economic activity and people’s livelihood alive? Can we actually put a value on the quality and quantity of years-of-life lost so that we can compare that with the economic loss suffered by the state or the country due to ongoing lockdown? Number of deaths by age group in New York City, one of the hardest hit areas of the country, reveals that death due to COVID-19 followed a lopsided distribution (Figure 3).

Figure 3: Death rate for COVID-19 in New York City as of June 21 by age group.
While loss of economic activity will affect the 18-64 age group the most, the risk of death toll is more concentrated in the 75-and-older population. Singer argued that the loss of economic activity will lower income potential of the age groups that are younger for decades, just like what happened during and after the Great Recession of 2008. Consequently, the quality of life of that population will be lowered for many more years. By doing lockdowns, the society could only save a limited amount of “quality life-years” of the elderly population at the cost of many more “quality life-years” of a larger population. Are we at a point when we need to think of tradeoffs between lockdown and increased deaths due to pandemic just like the doctors in Italy had to determine who should get the ventilators at the peak of the pandemic there? Everyone has the right to live, so can we really put a price tag on a human life? It is a very hard moral and ethical question, and the struggle and dilemma about this are currently on display in the United States.
Impact on Healthcare, Health Technology
The pandemic has rendered serious blows to the healthcare industry. For several months, hospitals canceled all elective procedures from which they made most of their money. This stalled their revenue generation. Clinics lost revenue as non-COVID-19 patients avoided clinic visits during this time. In the community health center space, many organizations saw about 30%-50% drop in revenue as patient flow ebbed drastically (based on data from California Primary Care Association).
Many healthcare organizations tried to switch to telehealth for nonemergency and non-COVID-19 patients. About 50% of physicians adopted telehealth at a rapid pace. Some states removed regulatory and payment barriers for telehealth visits, but that still wasn’t enough to save healthcare organizations from financial stress. At this time, many in the healthcare industry are still waiting for the stimulus support to keep their doors open. As the capital markets drastically slumped, venture capital slowed down after a record breaking first quarter with $3.1 billion investment in digital health companies. Health technology startups lost their sales pipeline and had to lay off workers. Based on a recent survey conducted by California-based Rock Health, the overall funding prospects look gloomy at this time for 2020 (Figure 4). There is a lot of global volatility, similar to what we are seeing in the topsy-turvy restarting of the American economy.

Still, There is Hope
Health technology is the future of the healthcare industry. That is a fundamental truth. The pandemic has shown again and again how unequipped the country is to tackle such a massive-scale healthcare crisis. Public health is often the most neglected area in the country, with little to no funding provided to overhaul the dilapidated technology infrastructure. Data interoperability, albeit better than a decade ago, is still a big challenge. Overly protective privacy barriers make rapid response difficult. Local and state leadership are realizing that. My hope is this pandemic will act as a catalyst that will eventually bring about the most desired investment and reform in the arcane regulatory framework in the coming years and will create opportunities for the new-age technology companies. Many of those companies are struggling now, but they are positioned to ameliorate the crisis and make sustained impact in the future.
Rajib Ghosh is the founder and CEO of Health Roads, LLC, a consulting company for enabling digital transformation in healthcare organizations. He has 25 years of technology experience in various industry verticals where he had management roles in software engineering, data analytics, program management, product management, business operations and strategy development. Ghosh spent a decade and half in the U.S. healthcare industry as part of a global ecosystem of medical device manufacturers, medical software vendors, telemedicine and telehealth solution providers. He’s held senior positions at Hill-Rom, Solta Medical and Bosch Healthcare. His recent work includes leading data-driven digital transformation in the public health space, including county-level healthcare agencies and organizations focused on underserved populations.
([email protected])