
November 14, 2022 in Healthcare Analytics
The Status of Universal Health Coverage and How Technology Can Help
SHARE: PRINT ARTICLE: https://doi.org/10.1287/LYTX.2022.06.06
https://doi.org/10.1287/LYTX.2022.06.06

On December 12, the world will celebrate Universal Health Coverage Day – the annual rallying point for advocates to raise their voices and share stories of the millions of people still waiting for healthcare, call on leaders to make smarter investments in health, and remind the world about the imperative of universal health coverage (UHC). It also marks the anniversary of the United Nations’ historic and unanimous endorsement of universal health coverage in 2012. Universal health coverage lifts people around the world out of the misery of an endless struggle to get access to quality healthcare and other human services without financial hardship. As we celebrate this year’s UHC Day, let’s take a look at how commitment from world leaders and technology can help us achieve meaningful progress toward the goals of UHC. After all, health for all (#Health4All) is an important initiative as we face the interlocked health, humanitarian and climate crisis around the world.
Preamble
In 2012, the U.N. unanimously endorsed a historic resolution urging all countries to accelerate progress toward UHC as an essential priority for international development. The call to action to all global leaders was to ensure that every human being could enjoy the highest attainable standard of physical and mental health regardless of race, religion, political belief or socioeconomic conditions. A big emphasis was given to understanding and incorporating social determinants of health in designing appropriate initiatives to achieve the goals of the resolution. Beginning in 2014, the Universal Health Coverage Coalition has celebrated UHC Day each year on December 12. This year’s UHC Day will be the last celebration before the U.N. High-Level Meeting on UHC takes place in 2023 and sets momentum toward achieving UHC by 2030.
Key Aspects of UHC
Affordability for receiving quality healthcare is still a major problem around the world. In developing and underdeveloped countries, healthcare infrastructure remains inadequate. This came to the surface during the COVID-19 pandemic. Investments in prevention of communicable diseases, vaccine development, distribution and administration are lagging, and because of that, we have seen the resurgence of new dangerous COVID-19 variants causing new waves of the disease. Food insecurity and housing issues plagued people in underdeveloped countries, causing major obstacles to health and nutrition. The Russia-Ukraine war has cut grain production in Ukraine by about 41%, leading to fear and prediction of large-scale food insecurity and perhaps starvation in many countries, especially in the developing world, this winter and into the next year. In developed nations, including the United States, affordable healthcare is still not in the reach of many. Universal health coverage is far from a reality – even in the U.S. – for myriad reasons. Income inequality, housing crisis and skyrocketing costs of healthcare have caused inequitable access to healthcare. Decades of underinvestment in healthcare technology infrastructure caused a major fiasco during the COVID-19 pandemic as the data collection and sharing – crucial for timely medical intervention – became a bottleneck. Political beliefs caused vaccine uptake to become uneven among different states. The U.S. suffered the worst human toll with more than a million deaths due to COVID-19. UHC, therefore, is applicable worldwide and not constrained to any specific region.

Figure 1. Healthcare outcomes ranking of the United States' health system compared to 10 other high-income countries in 2021.
Figure 1 illustrates a discouraging situation for the U.S. in terms of achieving better health outcomes. As the richest nation on earth, the U.S. has ranked 11 among the high-income nations in terms of healthcare outcomes based on 2021 data from the Commonwealth Fund. This, however, is not a surprise and proves that much in U.S. healthcare needs to change to address this situation.

Figure 2. Percentage of healthcare access measures for which members of select ethnic groups had better or worse access to care than the white population in the U.S., 2017-2019.
In the U.S., access to healthcare is quite uneven, as depicted in Figure 2. No ethnic or racial groups experienced better access to healthcare (across different access measures from health insurance to usual source of care) compared with non-Hispanic/white or white communities in 2017, 2018 or 2019. The Asian population, when compared with white populations, experienced better access on two measures (or 14%) but experienced worse access on four measures (or 29%).
When it comes to other countries around the world, we notice in Figure 3 that there is a high level of dissatisfaction among the population of countries across the board, from high-income to middle- and low-income countries. In many countries, the origin of the dissatisfaction is rooted in lack of access to affordable and quality healthcare.
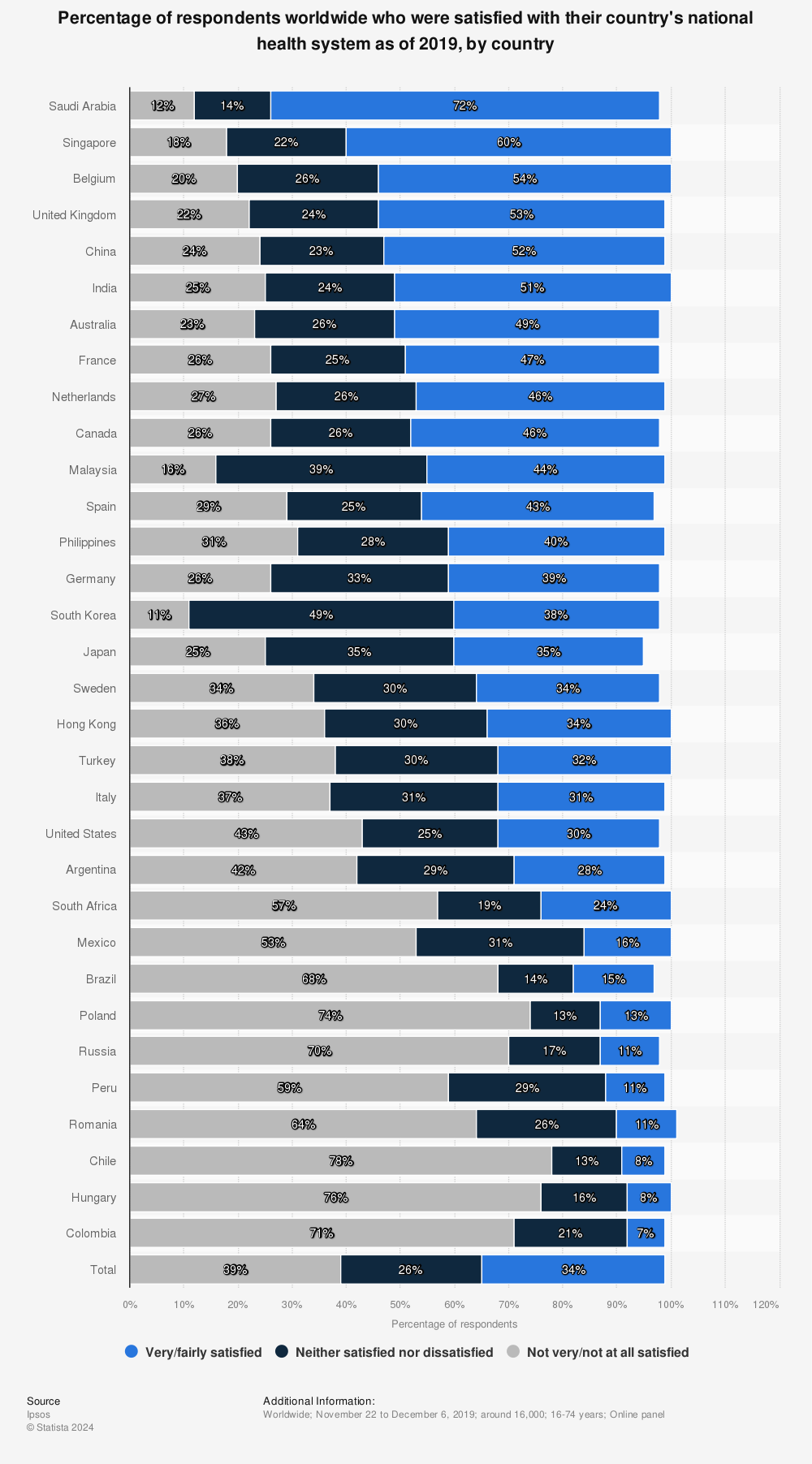
Figure 3. Level of satisfaction with national health systems worldwide as of 2019, by country.
Clearly, world leaders need to do more to make the goals of UHC a reality by 2030. There is not much time left. Technology needs to play a major role in democratizing healthcare. In many countries, technology (rudimentary and sophisticated) is already making a difference in people’s lives.
Technology and UHC Goals
For a long time, devices such as portable ultrasounds have helped in the diagnosis of conditions in many countries with remote or rural areas that are devoid of traditional healthcare facilities. Mobile devices, cloud and artificial intelligence have allowed rapid detection of communicable diseases such as HIV and Ebola. Mobile devices with apps have streamlined data collection and administrative processing in countries, allowing them to move away from error-prone paperwork and opaqueness of disease prevalence. Children born outside hospitals can be counted in Uganda and Nigeria with the help of SMS, and delays for getting HIV test results could be cut from 66 to 33 days on average in Malawi and Zambia. During the COVID-19 pandemic, many countries, including India and China, rolled out apps to track and warn people about potential exposure to the virus. The data was used to increase localized testing, diagnosis and disease control.
Although drugs are discovered and developed in the West first and then travel to other parts of the world, technology solutions do not necessarily follow suit. Many countries have unique circumstances that motivate them to look inward for technology solutions in creative ways. The goal is the same as that of UHC: to make access to care as affordable and easy as possible. General Electric’s portable ultrasound is a great example of when technologists and healthcare workers came together to create an $8,000 portable system instead of ones that are not portable and cost $100,000 or more. Later, such plug-in devices were brought back to the U.S. and sold to many rural communities as well as in disaster-stricken areas. Technology innovations travel both ways – outward from the West as well as inward to the West. Technology could be a key tool for countries and their leaders to race toward UHC goals by 2030. However, that does not mean sustained commitment from world leaders is secondary. Political will and leadership are utmost needs for humanity to find its mojo in the context of healthcare. This December, let us all work together with that mantra in mind.
Rajib Ghosh is the founder and CEO of Health Roads, LLC, a consulting company for enabling digital transformation in healthcare organizations. He has 25 years of technology experience in various industry verticals where he had management roles in software engineering, data analytics, program management, product management, business operations and strategy development. Ghosh spent a decade and half in the U.S. healthcare industry as part of a global ecosystem of medical device manufacturers, medical software vendors, telemedicine and telehealth solution providers. He’s held senior positions at Hill-Rom, Solta Medical and Bosch Healthcare. His recent work includes leading data-driven digital transformation in the public health space, including county-level healthcare agencies and organizations focused on underserved populations.
([email protected])